Qin, S., Sheng, J., Guo, W., Zhang, X. Curative effect of CES as adjuvant therapy on elderly patients with chronic insomnia. Practical Geriatrics. 2013; Vol. 27, No. 5:399-402.
Funding Source, Location of Study or Author’s Affiliation
Department of Psychology, Jingzhou Mental Health Center, Jing-zhou, China
Device
Alpha-Stim®
Key Variables
Sleep, Depression, and Anxiety.
Objective
To observe the clinical effect of cranial electrotherapy stimulation (CES) combined with alprazolam on elderly patients with chronic insomnia.
Design
A group of 108 elderly patients with chronic insomnia were randomized into three groups as part of an 8-week treatment study. The groups include a (1) medication group (MED) that received only alprazolam, (2) a CES group (CES) that received only CES treatment, and (3) a combined treatment group (MED+CES) that receiving both alprazolam and CES. Treatment efficacy was measured by comparing baseline and post-treatment sleep latency, total sleep time, and sleep efficiency using the Pittsburgh Sleep Quality Index (PSQI). Anxiety and depression typically accompany chronic insomnia, and any change in levels of anxiety and depression pre- and post-treatment were measured using the Hamilton Anxiety (HAM-A) and Hamilton Depression (HAM-D) rating scales. Changes to patients’ symptoms were evaluated by two research physicians trained to a consistency kappa value of 0.87.
Primary Outcome Measure
Sleep
- quality
- latency
- duration
- measured using the PSQI
- a 19-item scale that measures sleep quality and disturbance over two weeks.
- translated into Chinese by Liu Xianchen et al. (1996) the reliability and validity of which has been recognized by Chinese university students and patients with insomnia, depression, and neuroses.
- the PSQI includes7 factors and 19 self-evaluation items, the range of scores for each factor are from 0-3.
- higher PSQI scores indicate poorer sleep quality.
Secondary Outcome Measure
Anxiety
- As measured by the 14-item HAM-A scale each item has a score range of 1-5 score.
- The reliability and validity of the HAM-A has been widely recognized in China since Bai, Ji & Chen’s (2018) translation to Chinese.
- HAM-A total score (i) < 7 indicates “No anxiety”, (ii) 7-13 “Possible anxiety”, (iii) 14-20 “Definite anxiety”, (iv) 21-28 “Definite and obvious anxiety”, and (v) ≥ 29 “Possibly severe anxiety”.
Depression
- as measured by the 17-item Hamilton Depression Rating (HAM-D) scale which has a maximum score is 52 and each item is scored between 0 and 4.
- a total HAM-D total score of (i) 0–7 is considered as being “Normal”, (ii) 8–16 suggesting “Mild depression”, (iii) 17–23 “Moderate depression”, (iv) scores over 24 indicative of “Severe depression.”
Key Inclusion Criteria
Insomnia
- meet diagnostic criteria for insomnia as specified in the Chinese Classification of Mental Disorders (CCMD-3).
- insomnia with > 6 months since the onset of symptoms.
- with sleep latency >30 minutes nightly.
- reduced actual sleep time of <6 hours every night.
- PSQI ≥8.
Age
- ≥ 60 years.
Key Exclusion Criteria
- Insomnia caused by another mental or psychiatric disorder.
- Severe heart, lung, brain, liver, kidney, or other organic diseases.
- Diagnosis of sleep apnea.
- Drug and alcohol dependence or abuse.
Protocol Summary
A mandated washout period of two weeks prior to the start of treatment and discontinuation of all medications including antipsychotic, antidepressant, antianxiety, and mood stabilizers during the 8-weeks of treatment.
Patients were randomly allocated into one of three groups: (1) CES, (2) MED, and (3) MED+CES. All patients were asked to keep a sleep diary and to record changes in sleep, including latency and total sleep time, and to estimate their sleep efficiency.
CES therapy was administered using Alpha-Stim and the device was used in accordance with the manufacturer’s instructions. Patients in the CES only group received daily treatment for 20 minutes each time for eight weeks. The MED group were prescribed daily oral alprazolam 0.2~0.8mg to be taken 30 minutes before sleep. The MED+CES group received the same CES treatment protocol and dosage of alprazolam as the CES only and MED only groups.
Device Application Protocol
CES therapy was administered using Alpha-Stim and in accordance with the manufacturer’s instructions. The current intensity was set to 10-500 μA and the frequency to 1.5 Hz. During treatment, patients were asked to sit and given the opportunity to self-calibrate the magnitude of the current until they felt a slight tingling sensation. The treatment was given once a day, for 20 minutes each time over a period of eight weeks.
Statistical Analysis Plan
Treatment efficacy was evaluated by comparing total PSQI score, sleep latency, sleep efficiency, total sleep time, total HAM-A and HAM-D scores before and after eight weeks of treatment. A reduction in the total PSQI score and sleep latency, and an increase in total sleep time and sleep efficiency was interpreted as an improvement in sleep quality. At the end of eight weeks of treatment, a reduction in total HAM-A and HAM-D scores from baseline was indicative of a reduction in anxiety and depression.
All data were analyzed using SPSS 11.0 statistical software and a significance level of p<.05 set for interpretation of results. Analysis of Variance (ANOVA) was used for significance testing of between group comparisons. The Student–Newman–Keuls (SNK) post-hoc test was used for pairwise comparison. Paired sample t-test was used for the measurement data within a group. All cases completed 8 weeks of treatment, and no cases withdrew from the study.
Results
Subjects
A total of 108 patients aged >60 years were allocated into three groups of 36. The CES only group had an average course of the disease of 4.78±3.14 years and included 18 males and 18 females aged between 60 to 75 years equating to a mean age of 67.88±4.38 years. Patients in the medication only group were aged between 60 to 78 years, with an average age of 66.21±7.36, and included 18 males and 18 females, with and an average course of disease of 4.83±2.62 years. In the combination treatment group 19 males and 17 females aged from 60 to 76 years with an average age of 67.65±4.81 years, and an average course of disease of 4.92±2.53 years were enrolled. No statistically significant differences at baseline were found between the subjects in the three groups in terms of age, gender, sleep efficiency, PSQI, HAM-A, and HAM-D (p>.05).
Data Analysis
Score across all three groups and measures were significantly reduced from baseline to the end of the eighth week of treatment (p<.05).
Sleep
Comparison of total PSQI scores from baseline to the end of the eighth week of treatment in all three groups was significantly reduced (p<.05). The reduction in total PSQI scores was greatest in the MED+CES group than in the CES only or MED groups (p<.05). The reduction in total PSQI score was higher in the MED group than in the CES only group (p<.05).
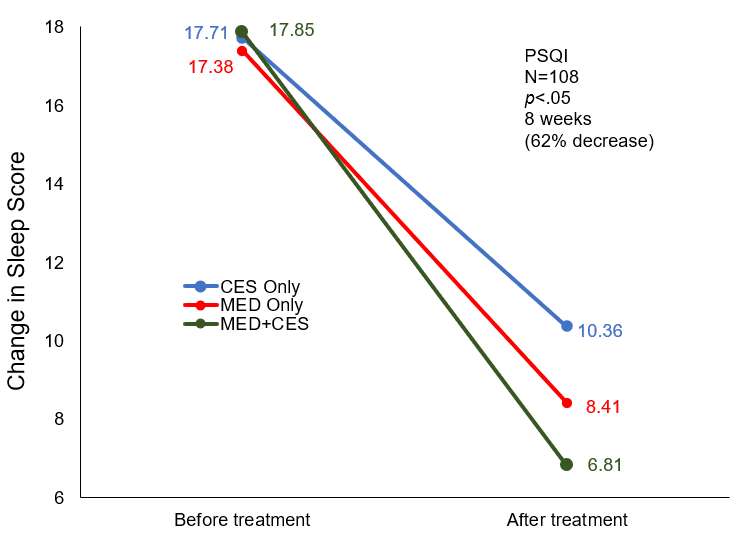
Change in sleep (PSQI) scores before and after treatment among the 3 groups.
Sleep latency, total sleep time, and sleep efficiency
After eight weeks of treatment, all three groups showed significant (p<.05) improvements in total sleep time and sleep efficiency, and significant reductions in sleep latency (p<.05). The increase in total sleep time and sleep efficiency was highest in the MED+CES group than the CES only or MED only groups (p<.05). Sleep latency was reduced more significantly in the MED+CES group than in the CES only and MED only groups (p<.05). Total sleep time and sleep efficiency increased more significantly in the CES only group than in the MED only group (p<.05). There was no significant difference between the CES only group or the MED only group (p>.05).
Comparison of clinical efficiency before and after treatment among the 3 groups
| Item | CES Only | MED Only | MED+CES | |
| Sleep latency (min) | Before treatment | 81.33±34.83 | 80.73±35.33 | 83.33±28.74 |
| After treatment | 33.16±11.31* | 33.65±11.38* | 24.06±8.23*# | |
| Total sleep time (min) | Before treatment | 216.71±43.41 | 222.50±58.98 | 229.38±46.51 |
| After treatment | 373.47±40.65* | 281.88±38.02*△ | 413.75±42.41*△# | |
| Sleep efficiency (%) | Before treatment | 45.04±17.24 | 45.12±18.22 | 43.34±17.48 |
| After treatment | 79.06±10.70* | 68.85±12.34* | 82.52±8.93* |
Note: Compared with before treatment, *p<.05; compared with the CES only group, △p<.05; compared with the medication only group, #p<.05
Anxiety and Depression
Compared with before treatment, the total HAM-A and HAM-D scores of the three groups were significantly reduced after eight weeks of treatment (p<.05). Reduction in HAM-A and HAM-D scores were greatest in the MED+CES group than those in the CES only and MED only groups (p<.05). The reduction in total HAM-A and HAM-D scores in the MED group were higher than those in the CES only group (p<.05).
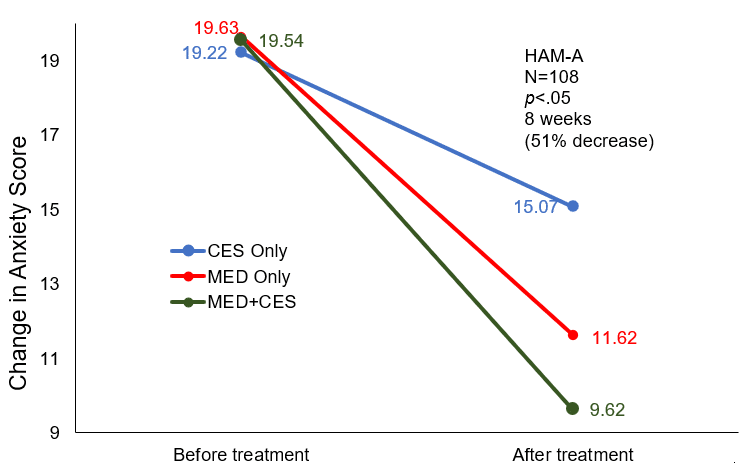
Change in anxiety (HAM-A) scores before and after treatment among the 3 groups.
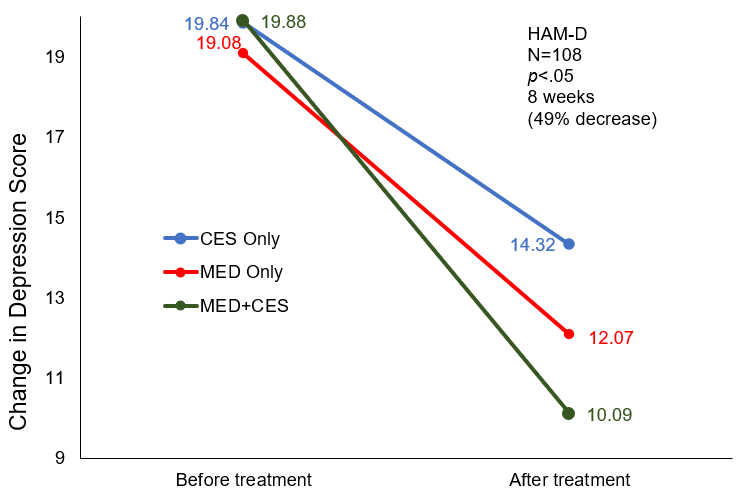
Change in depression (HAM-D) scores before and after treatment among the 3 groups.
Conclusion
The mainstay treatment for geriatric insomnia includes the use of benzodiazepines, which although effective are associated with greater adverse effects, risk of drug-drug interactions, and toxicity due to physiological changes associated with aging. Consequently, the need for non-medication treatments is urgently needed. In this study, CES or alprazolam – a common medication for sleep, were equally effective in treating geriatric patients with chronic insomnia. However, the results indicated that a combination treatment approach of CES and medication was significantly better at improving patients’ quality of sleep, reducing sleep latency, and increasing sleep duration, and perceived satisfaction with the level of reported sleep. In addition, combination treatment reduced the accompanying anxiety and depression symptoms more substantially.
The authors concluded that CES combined with alprazolam is the best treatment for elderly patients with chronic insomnia. Furthermore, the authors stated that they anticipate that once sleep improvements stabilized beyond the initial 8-week treatment cycle, that they would consider gradually reducing or discontinuing alprazolam, and developing a treatment plan focused on maintenance or consolidation using CES only.
Limitations
The study did not adhere to the recommended treatment guidelines for the use of Alpha-Stim CES as they set the frequency to 1.5 Hz rather than the recommended of 0.5 Hz. In addition, 20 minutes of daily CES treatment may not have been sufficient for patients whose comfortable current level was 200 uA or less. These deviations from recommended treatment guidelines may have impacted the results for the CES only group and the CES+MED group.
Study Quality: FAIR