Khyatee, S., Sarker,A., & Aggarwal R. Impact of Cranial Electrotherapy Stimulation Based Analysis of Heart Rate Variability in Insomnia. In: Prateek M., Sharma D., Tiwari R., Sharma R., Kumar K., Kumar N. (eds) Next Generation Computing Technologies on Computational Intelligence. NGCT 2018. Communications in Computer and Information Science, Vol 922. Springer, Singapore, 2019.
Funding Source, Location of Study, or Author’s Affiliation
Amity Institute of Physiotherapy, Amity University, Noida, U.P., India
Device
Alpha-Stim® AID
Key Variables
Sleep
Objective
Investigate the cross-sectional association between cranial electrotherapy stimulation (CES), sleep duration along with its quality and autonomic activity function in healthy individual utilizing two factors, the Global Pittsburgh Sleep Quality Index (PSQI) for evaluation of subjective sleep duration and quality and measuring beat to beat variation of the heart through heart rate variability.
Design
A randomized controlled trial on the impact of CES on HRV and insomnia. Patients that reported sleeping less than six hours were categorized as “Insomniac.” Patients were randomly allocated to the control and CES condition.
Primary Outcome Measure
- HRV measured by Physio Pack (Kubios 2.1).
- Sleep quality as measured by Global Pittsburg Sleep Quality Index (PSQI) score.
Secondary Outcome Measure
None reported.
Key Inclusion Criteria
- Diagnosis of Insomnia (Sleep <6 hours)
- Male or females >18 having:
- Regular night sleep.
- Normal basal metabolic index.
Key Exclusion Criteria
- Diagnosed with systemic or sleep disorders.
- Shift work.
- Pregnante.
- Regular daytime sleep/prolonged deviated sleep.
Protocol Summary
A pre and post-experimental study of patients diagnosed with insomnia were randomly allocated into two conditions, Control and Experimental (CES). Short-term HRV was measured by recording a five-minute ECG of each subject. HRV was assessed as per protocol. Sleep quality was measured by the global PSQI.
Device Application Protocol
After PSQI screening a set of instructions (i.e., to remain nil orally two hours before the test) was conveyed to the selected subjects. HRV was assessed with certain requisites such as removing any metal objects (including jewelry), being silent and relaxed with closed eyes lying Supine with palms facing upwards, without any physical movements. HRV examination room had an ambient temperature of 22 °C without direct light exposure to the subject. Alpha-Stim CES was given to participants in the Experimental group for five days per week for 20 minutes per day, over 21 days. The author does not discuss the current intensity used in this study.
Statistical Analysis Plan
Statistical analysis was done using SPSS software. Shapiro Wilk test was done to check normal distribution. Further, an independent t-test was used to check the differences between the two Clusters. A significance level of p<0.05 was adopted as a threshold for statistical significance.
Results
Subjects
A total of forty (40) males and females aged 18 to 44 years were screened and enrolled. Participants were randomly allocated into the Control and Experimental groups and categorized based on their sleep quality and duration and quality, the autonomic activity of 40 subjects was assessed with HRV for further analysis. No significant differences were reported at baseline between the groups.
Data Analysis
Geometric indices of Time Domain were significantly better in the Experimental group as compared to the Control, including STDHR, (p<.025), SDNN (p<.047), RMSSD (p<.048), RR Tri (p<.037), and TINN (p<.047). In the Frequency Domain Factors statistically, significant differences were found in VLF (p<.032), HF (p<.044), and Total Power (p<.045). Significant differences in favor of CES were reported on sleep quality and quantity as measured by PSQI and HRV as indicated by Physio Pack (p<.05).
The mean (SD) sleep quality and duration of the subjects before treatment in the Control and Experimental group were not significantly different. Baseline measures in the PSQI scores for quality for the Control group were 5.83±0.83 and 5.74±0.64 in the Experimental group. The mean (SD) sleep duration in the Control condition was 5±1.02 and 5±0.40 in the Experimental condition. Post-treatment sleep quality and duration were significantly better in the CES condition (p<.05). The mean (SD) Global PSQI score in the Experimental condition was 5.76±0.56 and 2.05±1.19 in the control. With the mean (SD) for sleep duration of 5±0.90 for the CES condition and 7±0.40 for the Control.
| Baseline | Post-Treatment | |||||
| Factors | Sham Control |
Active CES |
p Value |
Sham Control |
Active CES |
p Value |
| Mean RR (ms) | 849±186.75 | 841.30±68.15 | n.s. | 851.04±78.11 | 870.8±149.6 | 0.833 |
| STD RR (ms) | 73.95±5.87 | 71.99±5.80 | n.s. | 72.99±5.60 | 71.10±11.66 | 0.825 |
| Mean HR (1/min) | 3.58±2.02 | 4.19±1.26 | n.s. | 4.54±1.12 | 4.86±1.02 | 0.025* |
| STDHR (1/min) | 41.12±27.16 | 48.25±11.14 | n.s. | 44.14±16.40 | 59.45±18.8 | 0.047* |
| RMSSD (ms) | 38.2±31.24 | 37.25±14.44 | n.s. | 39.72±19.4 | 51.92±27.29 | 0.048* |
| NN50 | 55.88±32.44 | 61.41±52.46 | n.s. | 68.42±54.62 | 92.6±61.44 | 0.156 |
| pNN50 (%) | 18.4±20.24 | 17.20±15.21 | n.s. | 18.20±14.24 | 28.22±21.28 | 0.195 |
| SBP (mm/Hg) | 9.59±5.88 | 10.69±2.61 | n.s. | 10.63±1.51 | 13.75±4.09 | 0.037* |
| DBP (mm/Hg) | 157.22±104.79 | 175.62±125.7 | n.s. | 165.6±68.7 | 228.25±78.40 | 0.047* |
| Values expressed in Mean±S.D.; n.s. (Not significant); * (Significant Difference p<.05); RR (mean of the RR intervals); HR (Heart Rate); STDHR (Standard Deviation of Heart Rate); SDNN (Standard Deviation of NN Intervals); RMSSD (Root Mean Square of Successive Differences); NN50 (Number of Pairs of Successive NN Intervals that differ by more than 50 ms); pNN50 (Proportion of NN50 divided by total number of NN intervals); RRTri (Triangular Index of RR intervals); TIN (Triangular Interpolation of RR intervals); ms (milliseconds). | ||||||
HRV pre and post-CES for control and experimental groups
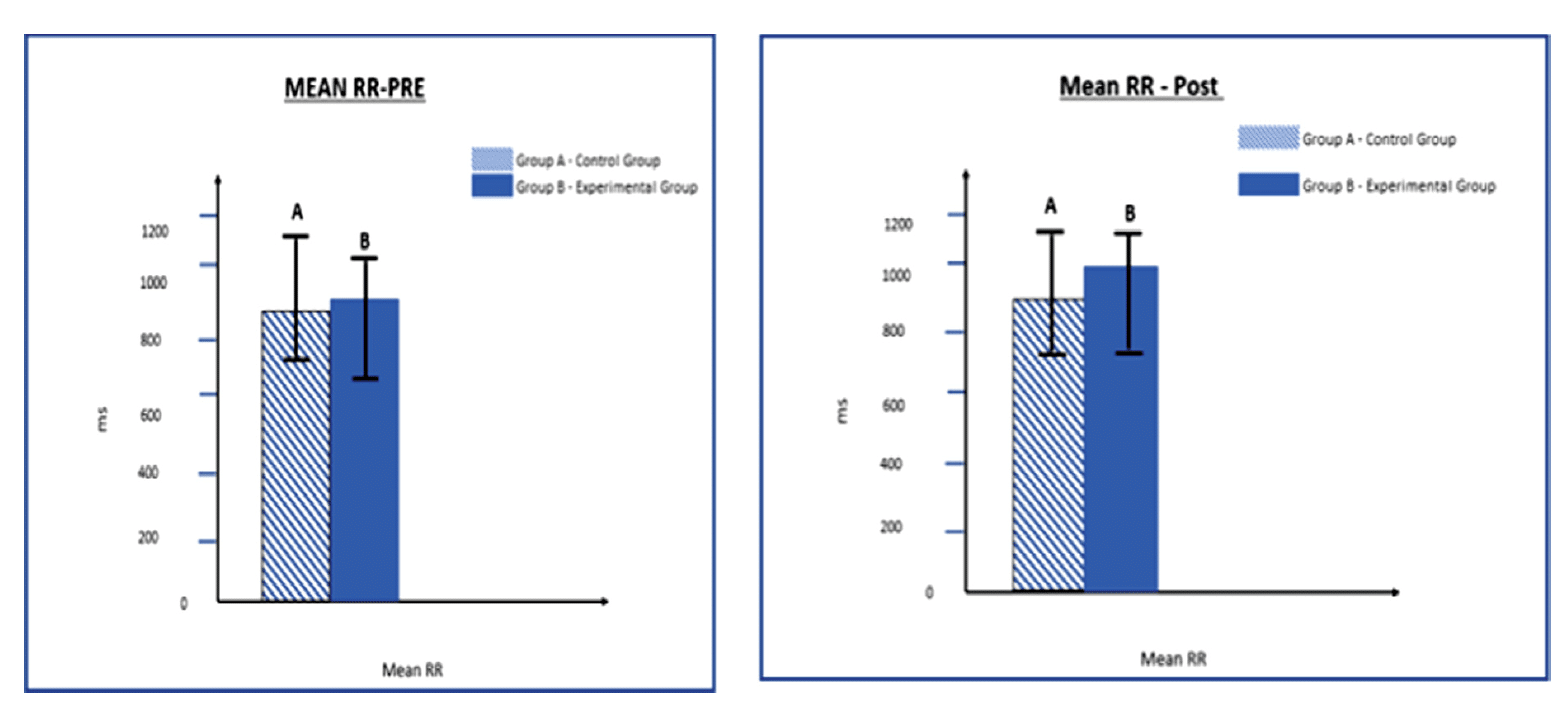
Mean of RR Interval Pre and Post for Control and CES Groups.

Mean Global Pittsburg Sleep Quality Score Pre and Post for Control and CES Groups.

Mean Triangular Interpolation of RR Interval Pre and Post for Control and CES Groups.
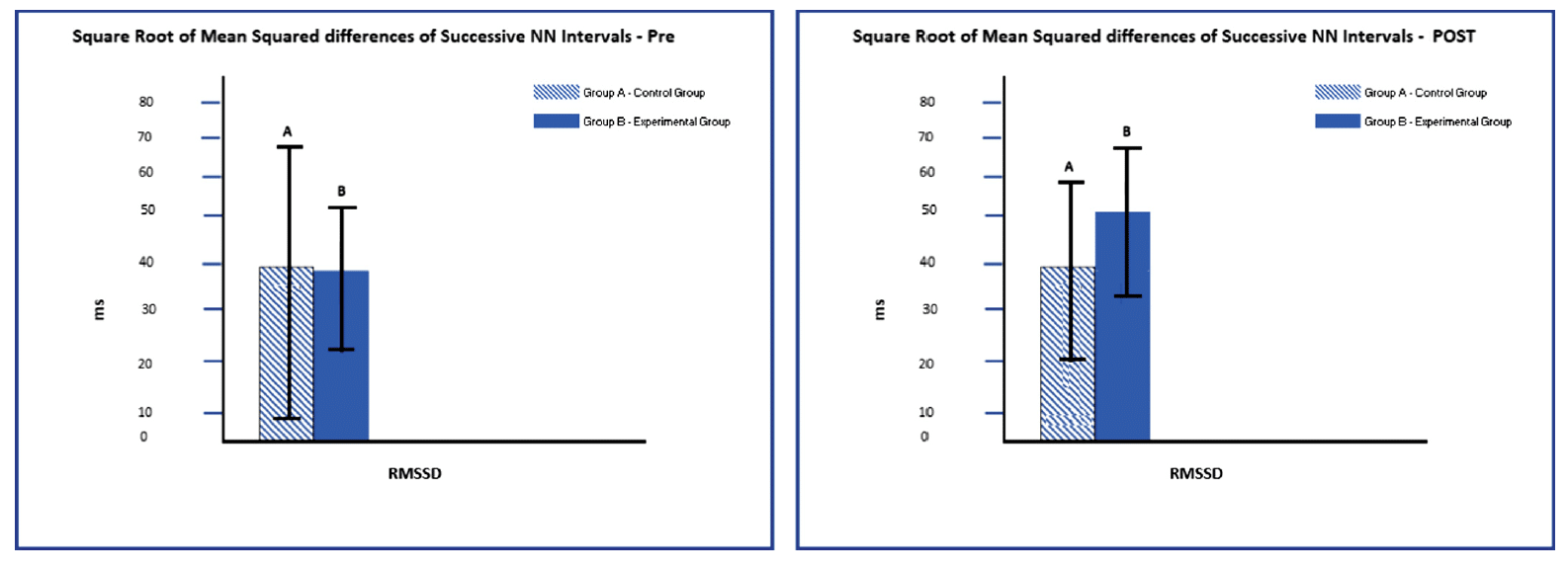
Mean Successive NN intervals Pre and Post for Control and CES Groups.
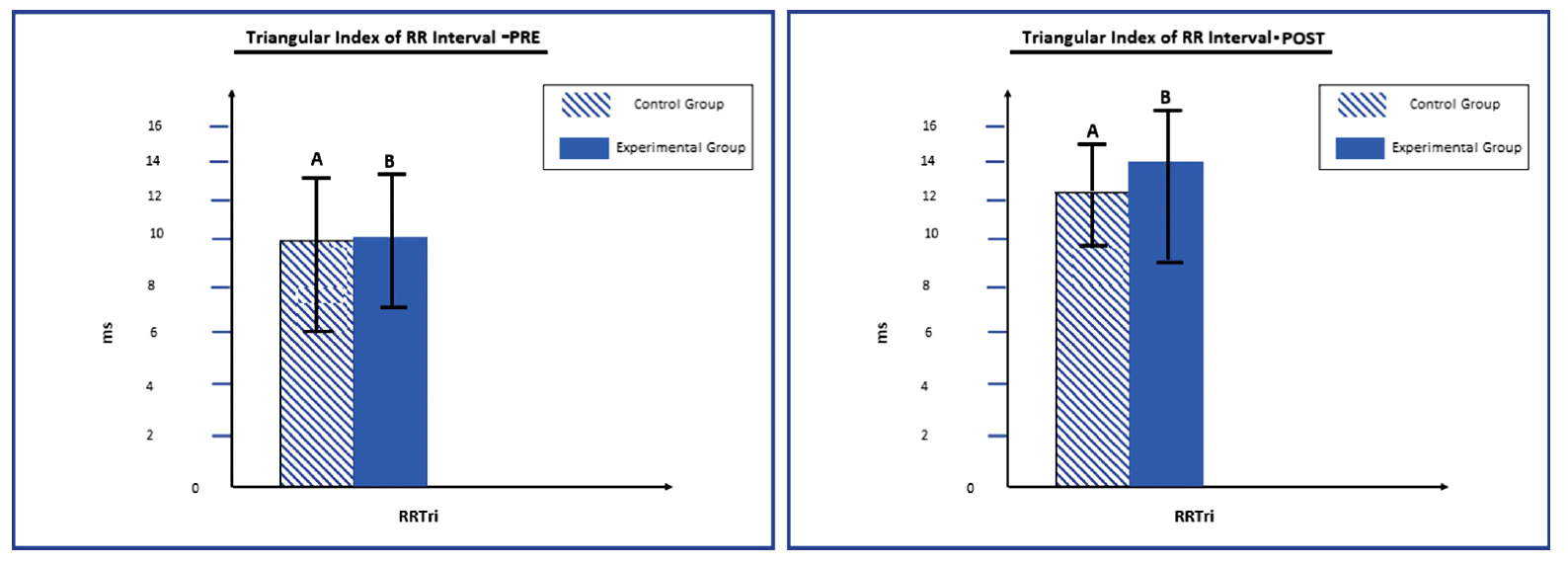
Mean Triangular Index of RR Interval Pre and Post for Control and CES Groups.
Conclusion
Poor quality and short duration sleep have an impact on HRV as associated with the nomic nervous function. HRV indexes (time, geometric, and frequency domain) from the first five minutes resting (supine) ECG data was increased in the CES condition, including RMSSD, TINN, and RRTri which defines the dominance of parasympathetic control with an increase of overall HRV, there was improved sympathovagal balance. An increase in HRV indexes is an indicator of improved sympathovagal balance and an increase of parasympathetic tone. CES stimulates cortical areas, subcortical areas, and cranial nerves in the brain. The authors propose a mechanism of action of CES supporting sympathovagal balance and parasympathetic dominance through regulation of the autonomic nervous system.
Limitations
The small sample size of this study limits generalizability of the findings. Replication of the study with a larger sample is warranted to better understand the mechanism of action of CES on HRV. While this was a good quality randomized control trial, the lack of double-blinding can potentially introduce bias into the interpretation of the results. The authors do not discuss a power analysis to determine appropriate sample size, nor do they discuss an apriori method of handling missing data.
Study Quality: GOOD